
I can’t remember much about the day when everything went wrong. No obvious moment indicated that the standard outpatient procedure would lead to weeks in the ICU, months in the hospital, and almost a year out of work.
Memories of a dark hospital room and slowly blinking lights come back in fevered fits. Dislocated voices from intrusive floating faces were saying that things would be alright.
I had known pain before: crutches, casts, and stitches. But until this moment, pain had always been experienced as something outside of myself. Now it was all that was left of me.
The day turned into night turned into day turned into night. I had given up on crying for the pain to subside. My soul had turned to the guttural moan of Job. Dear God, if this is my fate, may I never have been born at all.
I remember hearing the words “acute respiratory distress” and being moved to the ICU. I remember how my IV stand became a tree that blossomed with multi-colored ornaments hanging from stainless steel branches with cascading ripples of wires and tubes falling to my nose, arms, and chest.
Also hanging there was a clear plastic box containing a small bag marked hydromorphone—an opioid pain medication. The only moments that I remembered I was still a person and pain was an experience I was having—and not my entire existence—was the moment every 15 minutes when I pressed a small button that sent a pump whirring and boosted the normally slow trickle of the blessed, blessed, blessed analgesic already flowing.
Over the course of this medical odyssey, my 5’ 10” frame dropped below 130 pounds, the whites of my eyes turned yellow, my stomach became distended, fevers spiked and dropped. There was vomiting, diarrhea, hallucinations, surgeries, procedures, and minutes that turned into hours that turned to days when the doctors would not allow me to place even a chip of ice in my mouth.
There were crying family members surrounding the hospital bed, desperate phone calls to find a specialist who could handle my case, and the moment when I heard the doctor say the words “There is nothing more we can do.”
I had known pain before:
crutches, casts, and stitches.
But until this moment, pain had always been experienced as something outside of myself.
Now it was all that was left of me.
It was after all of this, when I was home, stable and recovering, that I learned I had developed a new complication. It was a disease related to some of the medication I had been and was still taking. Over two and a half million people struggle with this disease in the United States annually. It is an illness that has reached epidemic proportions in our country, claiming the lives of 78 people a day, with incidences of death quadrupling between 1999 and 2014, according to the Centers for Disease Control and Prevention.
The disease is opioid addiction.
My story of addiction is unremarkable. It was not the cause of my hospital stay but a result of it. I never doctor-hopped for pain meds or purchased them illegally. I never hit rock bottom, pawned my mother’s television set, or became a drug mule to pay for my habit. And by God’s grace, the disease was caught early.
During my journey of recovery, I came to understand more deeply than ever why addiction is called a disease. Some might think of an addict as a hard-living rock star who habituates their gluttony for an ever higher high, or an urban degenerate who feeds off the deepest depravities of human nature and becomes wealthy by destroying the lives of others. I discovered what many professionals have known for decades: that addicts aren’t “bad” people but those in the grip of something beyond their control.
What an Opioid Addict Looks Like
An opioid, from the root word opium, is a class of pain-relieving drugs that can vary in intensity from fentanyl (extreme) to codeine (mild). According to the Department of Health and Human Services, more than 240 million prescriptions were written for legal opioids in 2014—more than enough for every adult in the United States to have their own bottle. From 1999 to 2014, the period in which opioid overdose deaths quadrupled, so too did the sales of prescription opioids.
The widespread nature of the opioid epidemic that reaches across typical class, race, and geographical stereotypes has challenged myths of who drug addicts are. It has also widened the lens, revealing more moral actors participating in the crisis beyond the addict. Years of distorted public policy, overworked and undertrained doctors, intentionally misleading pharmaceutical marketing, and even watered down theology that reduces people to disembodied moral agents instead of whole human persons created in the image and likeness of a good God have all contributed through sins of both omission and commission.
Many opioid addicts began using these drugs for legitimate physical ailments, merely following their doctor’s orders. In fact, the American Society of Addiction Medicine reports that four out of five heroin addicts started with prescription opioid medications, with nearly all reporting that they eventually switched to heroin because of the price.
Our mental picture of an addict should include the high-school honors student who breaks her arm skateboarding and is prescribed an opioid by her doctor.
Or the middle-aged factory worker who has permanent back pain from his job and is prescribed an opioid by his overworked doctor who misses the fact that his patient is severely depressed.
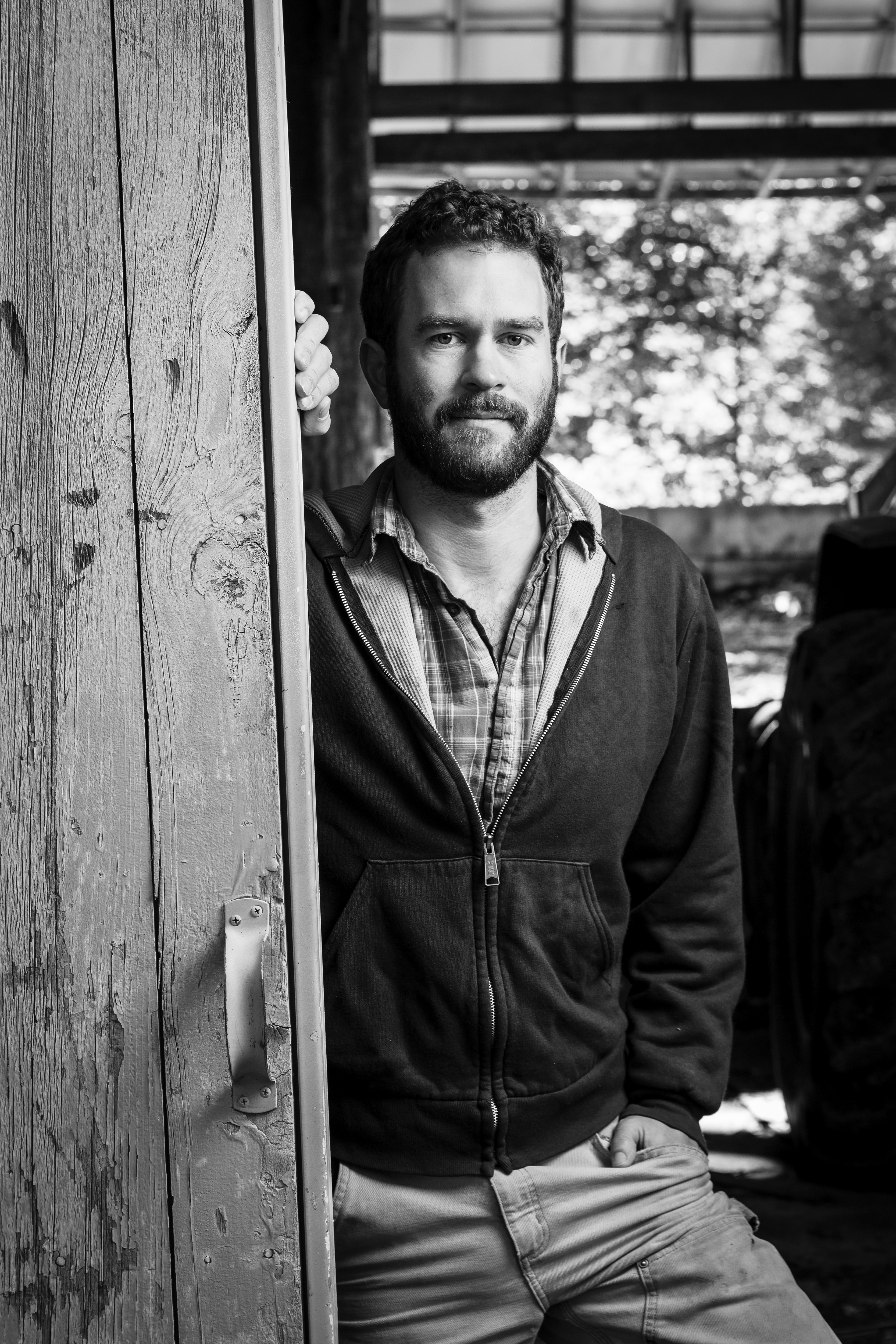
Or, think of me. A white, college-educated, employed, middle-class Christian from a good family who grew up on a farm in New Hampshire.
My complex medical history was the genesis of my addiction. In 2009, I suffered from acute necrotizing pancreatitis caused by a procedure commonly known as an ERCP. I was sent home with a PICC line, a sort of semi-permanent IV, in my arm. The IV connected me to a pump to receive most of my liquid and almost all of my nutrition for 12 hours a day. As I was able, I was supposed to slowly introduce into my diet clear liquids, then broths, then other easily digestible food.
Progress was slower than expected. I continued to experience pain with too much liquid. When I introduced light food, the pain would increase and I’d start vomiting.
During a follow up with my doctor, he determined that the cause of my ongoing pain and inability to eat was gastroparesis. The pain medicine I had been taking was deadening the nerve endings in my digestive tract and hindering my ability to process food. In other words, the pain medicine was now causing the pain. The more I took to relieve the pain, the more pain I felt.
That’s when my doctor told me.
“Tim, you need to know you are addicted to pain medicine.”
I felt my stomach drop and defenses rise as he said these words. All the stereotypes of addicts I didn’t think I held crept into my mind. Because I was legitimately in pain, I thought I couldn’t be an addict.
My doctor continued, “That isn’t a judgment on you. I’m not saying you’ve done anything wrong or that you aren’t still in pain. But we’ve been giving you this pain medicine for so long, your body is now dependent on it. It has gone from helping you to hurting you.”
I relaxed. I let my defenses down and loosened my grip on my justifications.
“I’m not going to just take the pain medicine away from you when you need it. But if I make that commitment to you, I want you to make a commitment to me. Will you take less whenever you can? For a while you couldn’t have made it without the pain medicine. Now to fully heal, you need to eventually stop taking it.”
I took a deep breath of relief. I wasn’t “bad.” I hadn’t done anything “wrong.” I had a new disease, a complication from my medication, and I had a doctor who was there and ready to help.
The Body and the Will
In July, Congress passed legislation to address the opioid crisis and heroin epidemic. Even the language of “crisis” and “epidemic” to describe the bill indicates a shift in mentality. The legislation acknowledges a growing medical consensus that the addict is subject to a disease—one with deep biological and psychological roots that often preclude individual choice.
This landmark legislation marked an important (albeit incomplete) step forward in reorienting public policy to reflect this new consensus. Framing addiction as chronic disease does not remove the moral choices involved but gives us a broader framework for understanding them. We can’t ignore the reality of our bodies, and when it comes to opioid addiction (and other addictions), part of the effect of those chemicals is to rewire the brain, making it more difficult or nearly impossible to change patterns of thought and behavior.
One commonly used analogy helping us understand addiction is heart disease. Like all analogies, it doesn’t explain everything, but it has the virtue of pointing out how clogged arteries cannot be cleared up by giving a pep talk to the patient or telling him to stop breathing so hard after climbing a set of stairs. Its causes are found in a mix of hereditary, environmental, and lifestyle choices.
It’s also helpful to think about how often our physical state and surroundings influence our actions. Have you ever had to apologize for something you said before you had your cup of coffee? Or maybe feelings of anger and impatience that you later realized were mostly resolved by eating a sandwich?
But the sense that addiction is solely a moral problem is hard to eradicate. After I clearly understood my addiction as a disease, I still battled internally with my self-image. I grew up with the “Just Say No” campaigns aimed at warning youth about illegal drugs. In that model, those with moral fortitude say “no,” and moral degenerates say “yes.” Those who said “no” received praise, and those who said “yes” were shamed and punished.
It Takes a Village of Grace
I removed the fentanyl patch first and switched to taking only Dilaudid. Within a day I could again feel my body in ways I did not realize I had been missing. At the same time, it felt as if a thick protective comforter had been ripped off from around me while I lay shivering and naked on my bed. Pain that had been blunted refocused and pressed out from the inside.
The doctor was right; I could handle the pain now without the same levels of opioids. But I couldn’t have continued my recovery if it were all up to the strength of my will alone.
Framing addiction as chronic disease does not remove the moral choices involved, but gives us a broader framework for understanding them.
My mother, a nurse, had been with me at that crucial doctor’s appointment. What would have happened if she had reacted with judgment instead of support? My employer at the time, Sojourners, had gone far above and beyond not just legal requirements but any general expectations to ensure I was financially secure, had access to quality health care, and had the hope of a job to return to. A friend who was starting a church in his living room picked me up on Sunday mornings. I was still taking pain pills to get through the service, but I stayed connected to a community defined by openness, honesty, mutual vulnerability, grace, and love.
So much more powerful than saying “no” to an opioid was the opportunity to say “yes” to a slow return to a life of flourishing.
As my body recovered and the pain subsided, I talked with my doctor and we stepped down from four-milligram to two-milligram pills. I began yoga and light exercise. Each step felt like a choice that rubbed against the grain of my body and mind.
I remember looking at a near empty bottle of pain pills and feeling nervous and insecure. I had switched to primarily over-the-counter pain relievers and one strong pain pill a day. When my doctor told me I could still get another refill if I needed it, I said no. I had determined that would be my last.
It was not an easy goodbye. The feeling was like the tremor in your hand when your blood sugar drops. Desire spreads out to every cell of your body as if each one is making its own demand, aching and promising to be satisfied with just a little more.
These feelings of withdrawal and the troubled sleep that came with them were intense for the first few days. Months later, they would flare up again as a reminder of what had been and the perilously thin line between me and the mounting numbers of long-term addicts and overdose victims.
I had to make the choice to recover from my addiction, but I could not have recovered without the choices of others. Many addicts also experience the reality that they would not have become addicts without their own choices, but they also would not have become addicts if not for the choices of others.
Addicts R Us
When I read story after story of tragic overdoses and the harm addiction can bring to communities and families, I no longer see the separation I once did. I see now that my story of addiction is not so far from that of a white addict living in rural West Virginia or black addict on the streets of Chicago. The origins of our use and the names of the substances might change, but our stories are fundamentally the same. Most addicts are addicts because their substance of choice really does do something for the pain they experience, whether that pain is physical, emotional, spiritual, or a mix of all three.
What I didn’t realize I needed to hear, and which my doctor affirmed, was that I was still a “good” person and I had an addiction. In a sense, I had not chosen to become an addict. Addiction had chosen me.
In struggling with my own sin, I have too often obsessed over Genesis 3 (the Fall) and functionally forgotten Genesis 1 and 2, which affirm that we are created good. And as Augustine, among others, has reminded us, while we might be born into sin, there is no power great enough to take away the fact that we have been made in the divine image.
I’ve realized that the word “addict” is a particularly useful descriptor for who I have always been. I always resonated with Paul’s lament: “I do not do the good I want to do, but the evil I do not want to do—this I keep on doing” (Rom. 7:19).
Some who have never experienced the furious grip of chemical dependence are tempted to split the world into “addicts” and “non-addicts,” morally bad and morally good. As I’ve said, I did not realize how fully I had embraced this view until faced with my own opioid addiction. Now, I realize that the world is divided between addicts who have begun to face their addictions and those who live under the illusion that they have none.
All who have come to the point where they acknowledge their own shortcomings and realize that they cannot eliminate them through their own power have admitted that they too, in their own way, are addicts. The addiction might be to food, shopping, status symbols, the need to be “right,” the need to be needed, or the need to feel moral superiority over those who struggle with less “societally acceptable” sins.
One of the most powerful teachings the church can embrace in light of this crisis is to say, “Let the one who is not an addict cast the first stone.”
While addiction science has made strides, there is still no silver bullet. Already there are stories of innovative addicts who have found new ways to abuse the medications intended to help them. Any approach that reduces addiction to a problem of brain chemistry and fails to acknowledge humans as moral actors will ultimately fail. But leading researchers and those discussing public initiatives have gone a long way to acknowledge the importance of a both/and methodology.
Churches can be cultural epicenters for shifts in societal norms. Our communities are built by and for wounded healers who recognize that no one is entirely free of addiction. It is in this weakness of each of us, and of the church as a whole, that Christ’s strength is made perfect.
The longer that addiction is seen as a struggle for the “sinners out there” and not at the heart of the struggle of each and every one of us, the longer this problem will make headlines and remain in the shadows. Sin takes its deepest root in the cover of darkness where it is never given a name. When our affliction is named for what it is and brought into the light, that’s when darkness may be overcome.
Timothy King is an independent communications and digital strategy consultant and helps his brother on their family’s farm in New Hampshire.